


When expectant parents hear the word Gastroshiza (often medically referred to as Gastroschisis) during a routine ultrasound, it can be an overwhelming and frightening moment. This congenital condition, characterized by a hole in the abdominal wall, causes a baby’s intestines to develop outside the body. While the sight of a newborn with exposed organs is distressing, modern medicine has made incredible strides in treating this condition. Today, the survival rate for infants born with Gastroshiza is remarkably high, often exceeding 90% in specialized care centers. Understanding the journey from diagnosis to recovery is the first step in navigating this medical challenge with confidence and hope.
What is Gastroshiza?
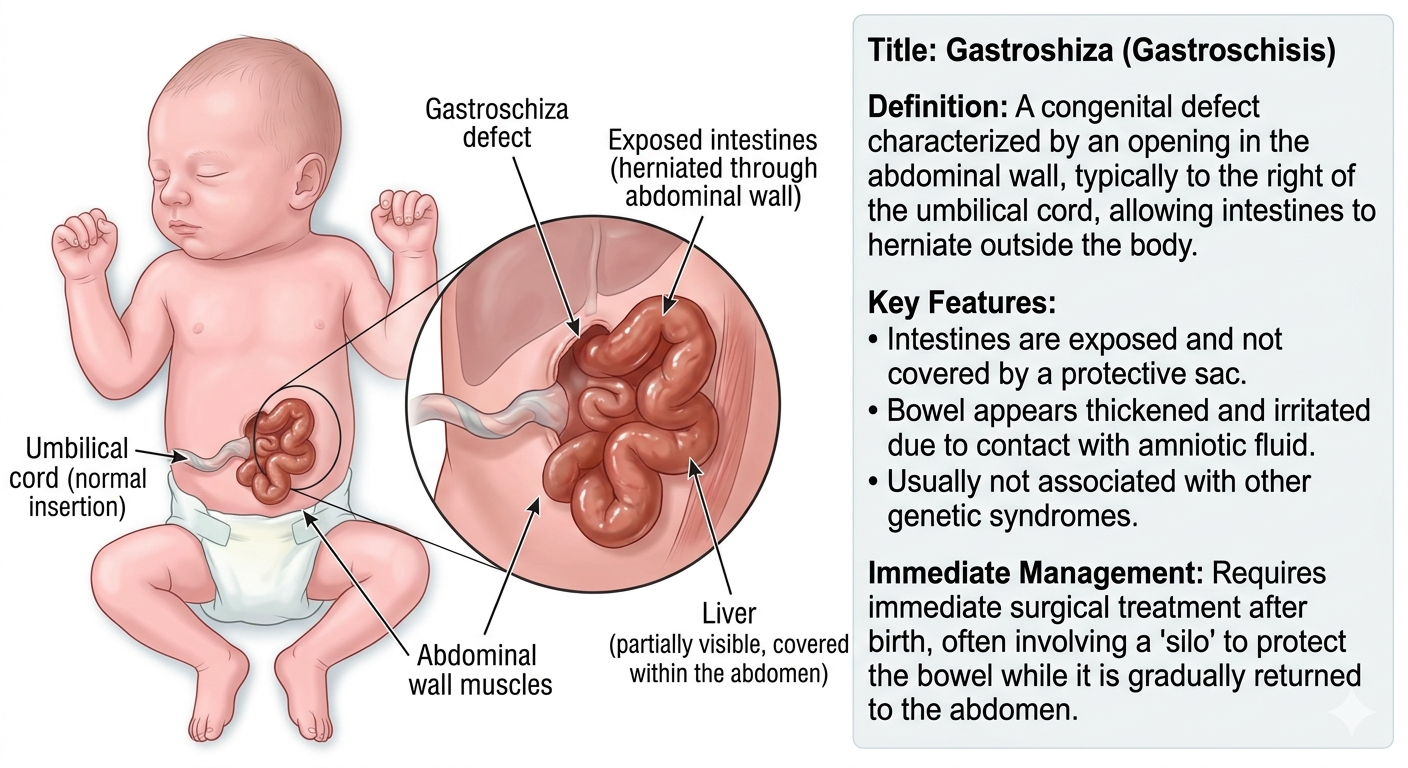
Gastroshiza is a birth defect that occurs early in pregnancy when the muscles of the baby’s abdominal wall do not fuse together correctly. This results in an opening, typically to the right of the umbilical cord. Because there is no protective sac covering the organs, the intestines—and sometimes the stomach or liver—protrude through this hole and float in the amniotic fluid.
Exposure to amniotic fluid can cause the bowel to become irritated, swollen, and thickened. This is why early detection and specialized delivery plans are so crucial. Unlike other abdominal defects, Gastroshiza is rarely associated with other genetic syndromes, meaning most babies affected are otherwise perfectly healthy.
Causes and Risk Factors of Gastroshiza
The exact cause of Gastroshiza remains a bit of a medical mystery, but researchers believe it stems from a combination of genetic and environmental factors. It typically happens around the fourth week of embryonic development. During this time, the abdominal wall is supposed to close, but for reasons not fully understood, a small gap remains.
Maternal Age and Lifestyle
Statistical data consistently shows that younger mothers, particularly those under the age of 20, are at a higher risk of having a baby with Gastroshiza. Other factors that have been linked to an increased incidence include:
-
Smoking or tobacco use during the early stages of pregnancy.
-
Exposure to certain environmental toxins or infections.
-
Low Body Mass Index (BMI) before pregnancy.
-
Use of certain medications or alcohol during the first trimester.
While these are known correlations, many cases of Gastroshiza occur in pregnancies where none of these risk factors are present. It is important for parents to understand that this is a developmental fluke and not a result of anything they did wrong.
Diagnosing Gastroshiza During Pregnancy
Fortunately, Gastroshiza is almost always detected before birth, usually during the second-trimester “anatomy scan” around 18 to 20 weeks. In some cases, it can be spotted as early as 12 weeks. Doctors look for free-floating loops of bowel in the amniotic fluid, which is a hallmark sign of the condition.
Prenatal Monitoring
Once a diagnosis of Gastroshiza is confirmed, the pregnancy is classified as high-risk. This doesn’t mean the baby is in immediate danger, but it does mean more frequent monitoring is required. Doctors will use regular ultrasounds to:



-
Monitor Growth: Babies with this condition sometimes experience Intrauterine Growth Restriction (IUGR).
-
Check Bowel Dilation: If the intestines look significantly swollen, it may influence the timing of the delivery.
-
Assess Amniotic Fluid Levels: Changes in fluid can signal stress for the baby.
The Delivery Process for Gastroshiza
Planning the birth is a critical part of managing Gastroshiza. Most doctors recommend delivering at a hospital equipped with a Level III or IV Neonatal Intensive Care Unit (NICU). This ensures that a pediatric surgical team is ready to act the moment the baby is born.
Vaginal Delivery vs. C-Section
Many people assume a C-section is mandatory for Gastroshiza, but that isn’t always the case. Many babies can be delivered vaginally if they are in the correct position and there are no other complications. However, doctors often choose to induce labor slightly early—usually around 37 weeks—to prevent further damage to the exposed bowel from the amniotic fluid.
Surgical Treatment for Gastroshiza
The primary goal after birth is to move the organs back into the abdomen and close the opening. Depending on the size of the defect and the condition of the intestines, surgeons will choose between two main approaches.
Primary Repair
If the amount of protruding bowel is small and the abdomen is large enough to accommodate it, a primary repair is performed. This surgery usually happens within hours of birth. The surgeon gently tucks the intestines back inside and stitches the abdominal wall closed.
Staged Repair (The Silo Method)
In cases where the intestines are very swollen or the baby’s abdomen is too small, a staged repair is necessary. Attempting to force the organs back in all at once could cause dangerous pressure on the baby’s diaphragm and heart.
-
The Silo: A clear plastic pouch called a “silo” is placed over the exposed organs
-
Gravity’s Help: Over several days, gravity and gentle manual pressure help the organs settle back into the body
-
Final Closure: Once the organs are safely inside, a final surgery is performed to close the gap.
Recovery in the NICU
Recovery from Gastroshiza is a marathon, not a sprint. Even after the surgery is successful, the baby’s intestines need time to “wake up.” Because they were exposed to amniotic fluid, they are often sluggish and unable to process food immediately.
Nutritional Support (TPN)
While waiting for the bowel to function, babies receive nutrition through an IV line. This is known as Total Parenteral Nutrition (TPN). It provides all the proteins, fats, and vitamins needed for growth.
Starting Feeds
The most significant milestone in the NICU is the “first feed.” Doctors look for signs that the bowel is working, such as the passage of stool or decreased stomach drainage. Feeds usually start with tiny amounts of breast milk or specialized formula delivered through a tube. It can take weeks, or sometimes months, for a baby with Gastroshiza to transition to full oral feedings.
Potential Complications of Gastroshiza
While the long-term outlook is generally excellent, some babies may face additional hurdles. It is important to be aware of these possibilities
-
Intestinal Atresia: In about 10% of cases, a portion of the intestine is missing or closed off, requiring further surgery.
-
Short Bowel Syndrome: If a large portion of the intestine is damaged and must be removed, the baby may have trouble absorbing enough nutrients.
-
Necrotizing Enterocolitis (NEC): This is a serious inflammation of the bowel that can occur in premature infants or those with abdominal defects.
-
Adhesions: Scar tissue from surgery can occasionally cause bowel obstructions later in life.
Long-Term Outlook for Children
Most children born with Gastroshiza grow up to lead completely normal, healthy lives. Once they overcome the initial challenges of the NICU and their digestive system stabilizes, they typically meet all their developmental milestones.
One unique “trademark” of a Gastroshiza survivor is their belly button. Depending on the surgery, some babies may not have a traditional navel, though surgeons often try to create a natural-looking one during the final closure. As they grow, these children can participate in sports, eat a regular diet, and have no lasting physical limitations.
Conclusion
A diagnosis of Gastroshiza is undoubtedly a major life event for any family. It requires a dedicated team of specialists, several weeks of intensive care, and a great deal of patience. However, the success stories are far more common than the complications. With early detection through modern ultrasound technology and the precision of neonatal surgery, babies born with their intestines on the outside are given every opportunity to thrive on the inside. If you are facing this diagnosis, stay focused on the milestones, lean on your medical team, and know that a healthy, happy future is the most likely outcome.
Frequently Asked Questions (FAQs)
1. Is Gastroshiza a genetic condition?
No, Gastroshiza is generally not considered a genetic or hereditary condition. It rarely runs in families and is seldom associated with chromosomal abnormalities like Down syndrome. It is usually a sporadic event that occurs during the early development of the fetus.
2. Can I breastfeed my baby if they have Gastroshiza?
Yes, absolutely. In fact, breast milk is highly recommended for babies with Gastroshiza because it is easier to digest than formula and helps protect the sensitive bowel from infection. While you may not be able to nurse right away in the NICU, you can pump milk which will be given to the baby via a feeding tube as soon as they are ready.
3. How long will my baby stay in the hospital?
The length of stay varies depending on the severity of the condition and how quickly the baby’s bowels begin to function. On average, babies with Gastroshiza spend between 4 and 10 weeks in the NICU. Some may go home sooner, while others with complications like intestinal atresia may stay longer.
4. Will my child need more surgeries in the future?
Most children only require the initial surgery (or series of staged procedures) shortly after birth. However, a small percentage may need follow-up procedures if they develop a bowel obstruction from scar tissue (adhesions) or if an umbilical hernia develops at the site of the repair.
5. What does the scar look like after Gastroshiza surgery?
The appearance of the scar depends on the surgical technique used. Many surgeons today use “sutureless” closure techniques or aim to hide the scar within a newly created belly button. Over time, the scar usually fades significantly and becomes a small reminder of the baby’s early strength






